There’s been a lot written lately about low risk chest pain and I thought I’d open a discussion about the HEART Score because it’s here.
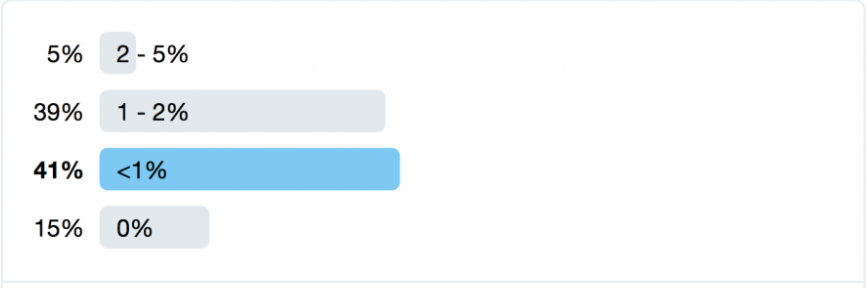
First, let’s review what we consider to be an acceptable miss rate for MACE (major adverse coronary event) within 90 days. In Canada, it seems like getting miss rates under 2% seems to be acceptable. Salim Rezaie from R.E.B.E.L EM asked this question on the Twitterverse and got this answer from a predominantly American audience.
Next, let’s all agree that almost every previous risk score has failed miserably including TIMI and the Vancouver rule.
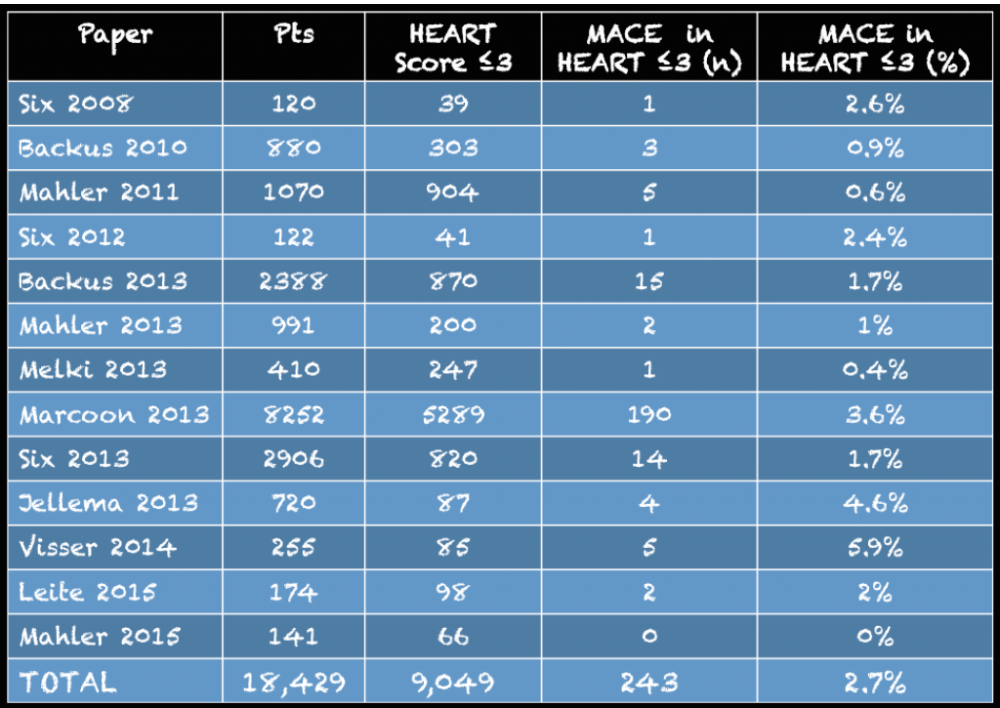
The initial studies on HEART were mixed, in the aggregate providing a miss rate of 2.7% for a HEART score of </= 3.
However, two external validation studies using modern troponins (not the new ultra high sensitive ones) in over 1000 patients have a miss rate of 0.8%.
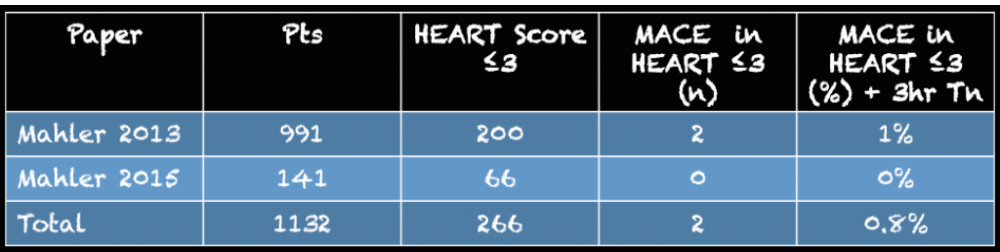
So, a score of </= 3 and two troponins 3 hours apart gets you to very low risk. Adding anything to this (including a stress test, CT coronary angiogram, etc) is very unlikely to lower your risk in a meaningful way and of course will lead to an increase in downstream testing from false positives.
The HEART Score can be found here.
There are a few caveats to using the HEART Score, as pointed out in the R.E.B.E.L EM Post on this talk:
(1) You can theoretically have a low risk score if your only abnormality is a positive Troponin. Most of us would not discharge home someone with chest pain and a Troponin of 5!
(2) A patient with ECG abnormalities could have a score </= 3. If these abnormalities are dynamic (ie you have a normal/different ECG previously), be careful.
(3) One of the things that gets you points is risk factors. If you never see a doctor it’s hard to have recognized risk factors.
But these limitations notwithstanding I think it’s a good ED based risk assessment tool for chest pain that allows us to send these patients home sooner.
Any thoughts?
Meant to respond to this a while ago and didn’t get around to it! I like it for low risk, but with anybody higher risk I find it probably would lead to MORE admissions and investigation like Tyler had mentioned.. i.e. a 65 year old who has had an MI before is automatically moderate risk (and therefore admitted?) even with normal EKG, and low suspicion story… What do you guys think about that?
I also think vs. the US we don’t do as much admitting/observing chest pain patients so I am not quite sure what we would do here with the moderate risk people.
I think HEART is meant to be used as a one way test for low risk patients.
The way I would employ is in low risk patients a 0 and 3 hour troponin allows you to safely discharge with good medico legal ammunition for the uncommon bad outcomes. There’s no reason to keep these patients 6-8 hours. I think this is where it helps us.
There is nothing in the score that says you have to admit the medium risk group. Maybe it just makes us slow down a little with those. Which I think is what we probably do already. I think we have been trained to be careful in 65 year olds with chest pain.
I definitely agree that Canadians will employ differently. The US is filled with risk averse MDs who admit everyone with chest pain.